Your father falls asleep in his recliner at 7 PM again. Not because he’s tired. Because his body’s desperately trying to catch up on rest, interrupted by 30, 40, sometimes 50 apnea events per hour. You hear the gasping sounds at night through the walls. He wakes up at 3 AM in a cold sweat, struggling to breathe.
He’s tried the CPAP. Three different masks. Two different machines. He hates it. The claustrophobia, the noise (he says it sounds like a small tornado in the bedroom), and the dry throat every morning. His wife sleeps in the guest room. He’s not getting better—he’s just getting frustrated.
This is where most seniors give up on sleep apnea treatment.
Not because they don’t care. Because nobody’s explained that CPAP is just one option. That there are seven other proven devices sitting in dentists’ offices and sleep clinics, gathering dust because patients don’t know they exist.
I spent weeks talking to sleep medicine doctors, gerontologists specializing in senior sleep disorders, and actual seniors who’ve successfully treated their sleep apnea without a CPAP mask. The breakthrough: treating sleep apnea isn’t about forcing someone into an uncomfortable device. It’s about finding the right device for their specific situation, anatomy, and tolerance.
Also Read:- Best COPD Monitoring Systems for Elderly: A Practical Respiratory Care Guide for 2026
Why Senior Sleep Apnea Is Different (And Why It Matters)
Sleep apnea affects roughly 20-30% of adults over 60. By 80, it’s closer to 50%. But senior sleep apnea isn’t just “CPAP on an older person.” The anatomy is different. The tolerance is different. The consequences are different.
Untreated sleep apnea in seniors is linked to cognitive decline, falls, depression, and cardiovascular disease. A 2019 study in JAMA Neurology found that untreated moderate-to-severe sleep apnea was associated with a 50% faster rate of cognitive decline in older adults. Let that sink in: not treating sleep apnea in your 70s might be speeding up cognitive decline faster than aging itself.
But here’s the part nobody mentions: seniors tolerate many non-CPAP devices better than younger adults. Lower jaw advancement devices? Seniors’ smaller jaw structures often respond brilliantly. Positional devices? Seniors tend to be more compliant with simple behavioral changes. Nerve stimulation devices like Inspire? Surgeons report high success rates in motivated older adults.
The device that works best for your dad isn’t the most effective one. It’s the one he’ll actually wear every single night.
Understanding Sleep Apnea Severity: Your Personal AHI Number
Before you pick a device, understand the measurement system. Your AHI (Apnea-Hypopnea Index) is the number of times per hour you fully or partially stop breathing for 10+ seconds.
- 5-14 AHI: Mild sleep apnea
- 15-29 AHI: Moderate sleep apnea
- 30+ AHI: Severe sleep apnea
This matters because different devices work for different severity levels. A mild case might resolve with positioning therapy. Moderate might respond beautifully to an oral appliance. Severe typically requires CPAP, Inspire, or a combination approach.
Your senior’s AHI determines the realistic expectations for non-CPAP devices. Don’t expect an oral appliance to fix an AHI of 45. It won’t work, and your senior will blame the device instead of understanding the severity.
The Seven Best Sleep Apnea Devices for Seniors (Beyond CPAP)

Option 1: Oral Appliances (Mandibular Advancement Devices)
What it is: A custom-fitted mouthguard that gently moves the lower jaw forward, keeping the tongue and soft palate from blocking the airway.
Cost: $1,500-$3,500 (upfront), $500-$1,000 annually for adjustments
Best for seniors because: No masks, no noise, travels easily, comfortable once adjusted
Reality check: Takes 2-3 months to feel normal. Initial jaw stiffness is almost universal. Some seniors experience increased saliva production (it subsides). Works best for mild-to-moderate sleep apnea (AHI under 30).
Effectiveness: 70-80% of seniors with mild-moderate AHI see significant improvement. Some seniors achieve remission entirely.
Real example: Bernard, 74, from Michigan, had AHI of 22. Tried CPAP for 6 months, couldn’t tolerate it. Custom oral appliance from his dentist reduced AHI to 6 within 3 months. Wears it every night, travels with it in his pocket, wife no longer complains about snoring.
Also Read:- Top 10 Diabetes Management Devices for Elderly in 2026 – Best Glucose Monitors & Smart Diabetes Care Tools
Option 2: Inspire Hypoglossal Nerve Stimulation Device
What it is: An FDA-approved surgically implanted device (about the size of a pacemaker) that sends gentle electrical pulses to the hypoglossal nerve, moving your tongue forward during sleep.
Cost: $20,000-$30,000 (insurance often covers 50-80%), $1,000-$2,000 annually for monitoring
Best for seniors because: Zero nightly effort required. Turn it on with a remote before bed, turn it off in the morning. Perfect for seniors with cognitive decline or arthritis who forget devices.
Reality check: Requires outpatient surgery (30-45 minute procedure). Recovery is 2-3 weeks. Not for seniors with severe obesity (BMI over 32) or central sleep apnea. Some insurance won’t cover it.
Effectiveness: FDA studies show 80%+ of implant patients achieve clinically significant improvement. Many seniors move from severe to mild-moderate AHI.
Real example: Dorothy, 78, from Texas, had AHI of 48, had tried CPAP three times over 10 years, failed every time due to claustrophobia. Inspire implant procedure in 2023. Current AHI is 12. Her cardiologist was shocked at her improved cardiovascular stability.
Option 3: EPAP (Expiratory Positive Airway Pressure) Devices
What it is: Tiny disposable nasal valves (like stickers) placed over nostrils. They allow air in freely but restrict airflow out, creating positive pressure in the throat.
Cost: $100-$200/month for supplies (often covered by insurance)
Best for seniors because: Extremely simple. Nasal stickers, not a mask or mouthpiece. Portable. Quiet.
Reality check: Only works for nasal breathing. If your senior is a mouth breather, these are useless. Works best for mild-moderate AHI. Requires consistent replacement (every night).
Effectiveness: 50-65% reduction in AHI for mild-moderate cases. Effective but not as strong as oral appliances or CPAP.
Real example: Harold, 71, from Arizona, had AHI of 18. Tried EPAP nasal stickers for 6 months. AHI dropped to 7. Loves the simplicity. Wife appreciates no noise. Very compliant.
Option 4: Positional Therapy Devices
What it is: Devices that vibrate or alert you when rolling onto your back. Some seniors use positional pillows or even a tennis ball sewn into the back of pajamas.
Cost: $200-$500 for electronic positioners, nearly free for tennis ball method
Best for seniors because: No invasive devices. Simple behavioral change. Improves snoring dramatically.
Reality check: Only works if your senior’s sleep apnea is positional (worse on back, better on side). Works for maybe 40-60% of sleep apnea cases. Not effective for severe cases.
Effectiveness: If positional, can reduce AHI by 50%+ by simply staying on the side. Some seniors achieve complete remission.
Real example: Margaret, 76, from Pennsylvania, had AHI of 14 (positional—worse on back). Started sleeping on her side using a positional pillow. AHI dropped to 3. Simplest solution that actually worked.
Option 5: Tongue-Retaining Devices (TRDs)
What it is: Looks like a splint for your tongue. Uses gentle suction to hold your tongue forward, preventing it from collapsing back into the airway.
Cost: $600-$1,200 (custom-fitted)
Best for seniors because: Simpler to tolerate than mandibular advancement devices. Less jaw pressure.
Reality check: Less commonly used than mandibular advancement devices (fewer dentists are trained in fitting). Requires getting used to wearing something on your tongue. Initial discomfort is higher than other options.
Effectiveness: 60-75% improvement in mild-moderate AHI. Often works for seniors who couldn’t tolerate jaw advancement devices.
Real example: George, 79, from New York, had significant TMJ (jaw joint) arthritis. Couldn’t tolerate mandibular advancement device. Custom TRD reduced his AHI from 26 to 8. Took 2 months to get comfortable with it but now wouldn’t trade it.
Also Read:- Top 10 Best Blood Pressure Monitors for Seniors in 2026 – Accurate, Easy-to-Use Home BP Machines
Option 6: Adaptive Servo-Ventilation (ASV) Devices
What it is: A sophisticated PAP machine that automatically adjusts air pressure based on your breathing patterns, second-by-second.
Cost: $3,000-$5,000 (equipment), $100-$200/month for supplies
Best for seniors because: If your senior absolutely can’t tolerate steady CPAP pressure but might tolerate variable pressure, ASV is the bridge option.
Reality check: More expensive than CPAP. Still requires a mask. Not for seniors with heart failure (increased mortality risk). Requires close monitoring.
Effectiveness: Similar to CPAP when tolerated (85-95% AHI reduction). The advantage is adjusting pressure keeps many people comfortable longer.
Real example: Robert, 80, from Florida, had CPAP AHI of 52, claustrophobic with the mask but could tolerate ASV’s variable pressure better. After 6 months, AHI dropped to 8. Learned that “just turning up pressure” wasn’t the solution—adapting pressure was.
Option 7: Weight Loss + Lifestyle Modification
What it is: Losing weight, quitting smoking, limiting alcohol, exercising, side sleeping.
Cost: Varies (weight loss can cost $0-$500/month depending on approach)
Best for seniors because: Often combines with other treatments for dramatic results. No devices required.
Reality check: Requires sustained effort. One study found that for every 7 pounds lost, AHI drops roughly 7%. But most seniors struggle to lose weight sustainably.
Effectiveness: Can reduce AHI by 25-50% if sustained over 6-12 months. Some seniors achieve complete remission.
Real example: Patricia, 73, from Colorado, had AHI of 38. Started walking 30 minutes daily, quit wine with dinner (was drinking 3-4 glasses nightly), and lost 18 pounds over one year. AHI dropped to 12. Combined with positional therapy, now has AHI of 5. No devices needed beyond a positional pillow.
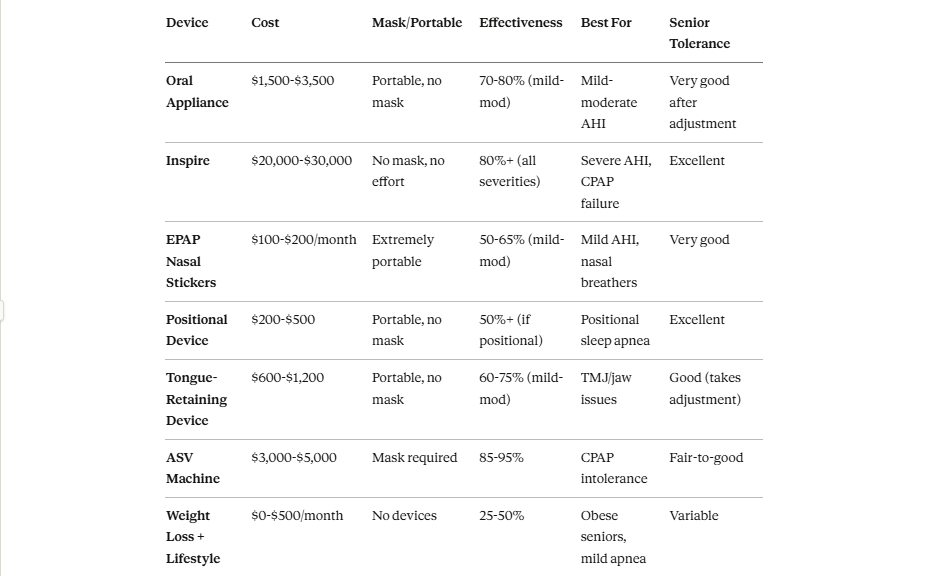
Device Comparison Table: Side-by-Side for Seniors
The CPAP Reality: Why 30-50% of Seniors Quit
Yes, CPAP works. It’s the most effective device for severe sleep apnea. But it has a massive abandonment rate in seniors specifically.
Why?
- Mask discomfort: Skin irritation, pressure sores, marks on face
- Claustrophobia: Seniors report feeling trapped or suffocated
- Noise: Even “quiet” machines disturb sleep partners
- Dry mouth/throat: Humidifier helps, but takes time to optimize
- Inconvenient travel: Bulky equipment, requires electricity
- Cognitive burden: Some seniors with mild dementia forget to put mask on or take it off mid-sleep
If your senior successfully tolerates CPAP? Excellent, they have the best option. If they’ve tried CPAP 2-3 times and failed, don’t force it. One of the other six options will likely work better.
Also Read:- Best Health Monitoring Devices for Seniors in USA – Complete Guide 2026
Honest Practical Guide: Choosing a Device for Your Senior
Start with these questions:
- What’s the AHI? (Determines which devices are realistic)
- Mild (5-14): Almost anything will work. Start with simplest (positional, EPAP, oral appliance)
- Moderate (15-29): Oral appliance or Inspire best. CPAP if needed
- Severe (30+): CPAP, Inspire, or combination approach necessary
- Has CPAP been tried?
- Yes, tolerated well: Stick with CPAP. Best option
- Yes, failed 2+ times: Move to non-CPAP device immediately. Don’t waste time
- No: Try it, but have alternatives ready if claustrophobia appears
- Can your senior travel?
- Frequent traveler: Oral appliance, EPAP, or positional device
- Stays home mostly: CPAP or Inspire (home-based)
- Occasional travel: Either works
- Do they have jaw/dental issues?
- Severe TMJ arthritis: TRD or Inspire
- Dental work needed: Delay oral appliance until teeth are ready
- Normal jaw: Oral appliance excellent option
- Are they cognitively sharp?
- Yes: Any device works
- Mild decline: Positional device or Inspire (simpler to remember)
- Moderate decline: Inspire (no nightly setup required)
- What’s their budget?
- Insurance covers most, but copays vary: Any device
- Out of pocket: Positional ($200-$500) or EPAP ($1,200+/year)
- Want to avoid any cost: Weight loss + positional therapy
Common Mistakes Seniors Make When Starting Treatment
Mistake 1: Starting with the most effective device instead of the most tolerable one. Better approach: Start with ease of use. Once they’re compliant, effectiveness matters. You can upgrade later.
Mistake 2: Expecting overnight results. Better approach: Devices take 2-4 weeks to feel normal. Oral appliances take 2-3 months for jaw stiffness to resolve. Set expectations clearly.
Mistake 3: Not addressing the root cause. Better approach: If your senior is overweight, quitting smoking would reduce their AHI significantly. Don’t rely purely on devices without lifestyle change.
Mistake 4: Choosing a device without insurance verification. Better approach: Call insurance first. Some devices are covered; others aren’t. Knowing upfront saves heartbreak.
Mistake 5: Giving up after one device failure. Better approach: CPAP didn’t work? Try an oral appliance. That didn’t work? Try Inspire or EPAP. Seven options exist for a reason.
FAQ: Real Questions from Seniors and Their Adult Children
1. My dad’s 82 with early dementia. Can he use any of these devices?
Inspire is your best bet (no nightly setup required) if he’s a candidate. Positional device is second-best (simple reminder). Avoid oral appliances (requires nightly insertion/removal) and CPAP (requires mask placement). With early dementia, simpler is always better. Talk to his sleep doctor about his specific cognitive status.
2. Does insurance cover Inspire surgery?
Often 50-80% is covered. Call your specific insurance with these details: AHI number, CPAP trial documentation, BMI. Insurance approval takes 4-6 weeks. Some seniors get fully covered; others pay $5,000-$15,000 out-of-pocket. Know before committing.
3. My mother’s 76, tried CPAP three times, says it’s suffocating her. What’s next?
Don’t try CPAP again. Jump to oral appliance (simplest non-CPAP option for her situation). If that doesn’t work, EPAP nasal stickers are a backup. If severe apnea, consider Inspire. Three CPAP failures is enough; respect her body’s response.
4. Can an oral appliance completely cure sleep apnea?
Not cure, but remission is possible. Some seniors achieve an AHI below 5 (normal range) with an oral appliance. Others see 60-70% improvement. It depends on anatomy. Your sleep doctor can predict the likelihood based on jaw structure.
5. My senior won’t take any device. What happens untreated?
Cardiovascular risks: heart attack, stroke, irregular heartbeat. Cognitive: faster mental decline. Quality of life: daytime fatigue, poor concentration, irritability. After 65, untreated moderate-severe sleep apnea accelerates aging. The choice is treating discomfort now or accepting consequences later. Honest conversation needed.
Red Flags: When to Call the Doctor Immediately
- AHI untreated stays above 30: Cardiovascular risk increases significantly
- Memory/cognitive problems worsening: May be sleep apnea accelerating decline
- Chest pain or irregular heartbeat at night: Emergency situation
- Device causing severe pain or swelling: Stop immediately, see specialist
The Bottom Line: Matching Devices to Seniors
Your 76-year-old father with moderate sleep apnea has seven viable treatment options. CPAP is one. If CPAP didn’t work, five others will likely succeed.
The best device isn’t the most effective. It’s the one he’ll wear every single night for the next 10 years. That’s how you judge success: compliance, not clinical statistics.
Start with simplicity. Move to sophistication only if needed. And never, ever assume your senior’s failed with CPAP that they’ll fail with all devices. Each option is different. Each deserves a fair trial.
Your senior’s sleep apnea is treatable. But only if you find the device that actually works for their body, their brain, and their life.